
March 14, 2026 • By Dr. Sadok Derouich
Should EMR software be country-specific? The case for borderless medical software
The technology to build truly borderless medical software already exists. What has been missing is the product philosophy to do it.
No — and the technical barriers to building country-agnostic medical software have largely disappeared. What keeps EMR software country-specific today is not technology but business decisions, legacy architecture, and a failure to design with global constraints from the beginning. Every argument for country-specific medical software has a modern counter — and the tools to build genuinely borderless healthcare products exist right now.
In an analysis of why Western EMR software fails overseas, we established the problem: most EMR platforms were built for Western healthcare systems and left the majority of the world's doctors without tools designed for their reality. This article answers the natural next question: should we build differently — and if so, how?
What you will learn in this article:
- The 6 honest reasons why EMR software became country-specific — and why each one made sense at the time
- Why none of those reasons holds the same weight in 2026
- The concrete architectural decisions that make a medical office app truly borderless from day one
- Why building for a larger global market also produces better economics for everyone
- Why the missing ingredient is not technology but the rare combination of clinical and technical expertise
Medical Insight
When I decided to build doctoLys, the first and most important architectural decision I made was this: the product would have zero country dependencies. No billing module. No insurance integration. No assumption about where data should live. I made this decision not because I had a grand global vision — I made it because I was a doctor in Tunisia who had just spent weeks trying to find software that worked for me, and found nothing. Building for my own context meant building for everyone the market had ignored.
Why EMR software became country-specific — 6 honest reasons
Before arguing that country-specific EMR is no longer necessary, it is worth being honest about why it happened. Each of these reasons was rational at the time.
1. Regulations appeared country-specific on the surface. HIPAA in the US, GDPR in Europe, PDPA in Thailand, POPI in South Africa — the names were different, the legal frameworks were different, and the compliance requirements appeared to demand locally-adapted products.
2. Interoperability tied systems to national infrastructure. Insurance billing, social security platforms, national lab networks, patient portals — these varied by country and required deep integration. Building a product that connected to France's CPAM system meant building something that did not work anywhere else.
3. Sales models required local representatives. Enterprise software was sold, not adopted. Local sales teams understood local regulations, spoke the local language, and built the relationships necessary to close deals with hospital procurement departments.
4. Pricing and add-ons were adapted per market. Healthcare software pricing in the US reflected what US practices could afford. The same product architecture exported to a developing country market required different pricing tiers, different payment methods, and different add-on structures.
5. Clinical needs were assumed to be homogeneous per country. Software vendors built for their primary market and assumed that doctors within that market had similar needs. The idea that a GP in Tunisia had the same core clinical needs as a GP in Vietnam — regardless of country — simply was not part of the product thinking.
6. Most platforms were built before the cloud era. Software built in the 1990s and 2000s ran on local servers. Data literally had to live in a specific physical location. Country-specific architecture was not a design choice — it was a technical constraint of the infrastructure available at the time.
Why none of these reasons holds the same weight in 2026
This is where the argument gets interesting — because every one of the above reasons has a modern answer that did not exist when most of these platforms were built.
Regulations: convergence, not divergence
The surface appearance of regulatory difference masks a deep structural similarity. HIPAA, GDPR, PDPA, and most national healthcare data laws converge on the same core requirements: data encryption at rest and in transit, access controls and audit trails, patient rights over their own data, breach notification, and data integrity guarantees.
The real divergence is narrower than it appears: primarily data localization — the requirement that patient data be stored within national borders. This is a genuine constraint, but it is an infrastructural one, not an architectural one. Modern cloud providers offer data residency in dozens of countries via regional deployments. A medical office app built with data localization in mind from the start can comply with any national sovereignty law without touching a single line of application code.
A 2024 analysis of global healthcare data regulations confirmed that while frameworks differ in name and enforcement, the underlying patient protection principles are remarkably consistent across jurisdictions.
Interoperability: FHIR changed everything
The argument that interoperability requires country-specific architecture was valid before the emergence of global standards. It no longer is.
FHIR (Fast Healthcare Interoperability Resources) has become the global standard for healthcare data exchange — a RESTful API specification that defines how any system can communicate with any other, regardless of country. As of 2025, FHIR is actively used in healthcare systems across every major region.
What this means in practice: connecting a borderless medical office app to a national lab system, a social security platform, or a patient portal is now an API integration project — not an architecture project. It takes hours, not months, and does not require rebuilding the core product for each new market.
| Feature | doctoLys | Country-specific EMR |
|---|---|---|
| Regulatory compliance | Configurable per deployment region | Hardcoded for one jurisdiction |
| Interoperability | FHIR API — connects to any national system | Built-in integration for one national system only |
| Data location | Per-tenant database, any cloud region | Fixed server location, single jurisdiction |
| New market entry | Configuration — hours | New product build — months or years |
| Onboarding | Self-serve with AI assistant | Local sales rep required |
Sales demos: a symptom of complexity, not a necessity
The requirement for a sales demo is not a feature of medical software — it is a symptom of excessive complexity. If a product requires a trained representative to explain it, the product is too complex.
A 2022 study on EMR adoption in Nigeria found that perceived usefulness had an odds ratio of 18 on adoption — meaning that when doctors could immediately experience value, they adopted. The demo exists to create that experience artificially for products that cannot create it naturally.
Simplify the product so that value is immediate, and the demo becomes unnecessary. Add an AI onboarding assistant to guide the first consultation, and the local sales representative becomes redundant entirely. This is not a theoretical position — it is how doctoLys was designed, and why a doctor in Dakar can be fully operational in under 5 minutes with no human intervention.
Pricing: a global market enables better economics for everyone
The argument that pricing must be adapted per country assumes that the product carries a cost structure requiring high pricing. A mobile-first, cloud-native medical office app with no physical infrastructure, no local support team, and no implementation cost can be priced at $19/month globally.
But the economics argument runs deeper than this. A medical software company that limits itself to the US or European market is voluntarily ignoring an addressable market of hundreds of millions of physicians worldwide. Targeting a truly global market — including the 80% of the world's doctors who are currently underserved — dramatically expands the total addressable market (TAM). A larger TAM allows the developer to invest more in the product, offer better pricing, and build the kind of support infrastructure that makes the product better for everyone — including doctors in developed markets.
Country-specificity is not just a barrier to access. It is a business model that leaves value on the table for both the user and the developer.
Homogeneous needs: by role, not by country
This is the most important nuance in the entire argument. Clinical needs are not homogeneous by country — they are homogeneous by clinical role.
A solo GP in Tunisia, Vietnam, Colombia, and Norway has the same core clinical needs: open a patient file, record consultation notes, write a prescription, track follow-ups. What differs between these doctors is not the clinical workflow — it is the administrative and billing context layered on top by their respective national healthcare systems.
The insight that makes borderless medical software possible is recognising which features are universal clinical needs and which are local administrative artifacts. Stripping the latter out of the core product — and making them configurable rather than hardcoded — is what unlocks universality.
The person who can make this distinction reliably is not a software engineer alone, and not a clinician alone. It requires someone who masters both — who understands clinical workflows deeply enough to know what is universal, and understands software architecture well enough to implement configurability at scale. We explore this idea further in an upcoming article: how a doctor-led development team builds better clinical architecture.
Medical Insight
The clearest example of this in building doctoLys was the medication list. In France, the standard formulary is the Vidal. In Tunisia, it is different. In Nigeria, different again. A country-specific product hardcodes the local list. We made it user-configurable from day one — the doctor builds their own. The architecture is the same everywhere. The content is local. This one decision unlocked dozens of markets without writing a single line of country-specific code.
The technical blueprint: what borderless medical software looks like in practice
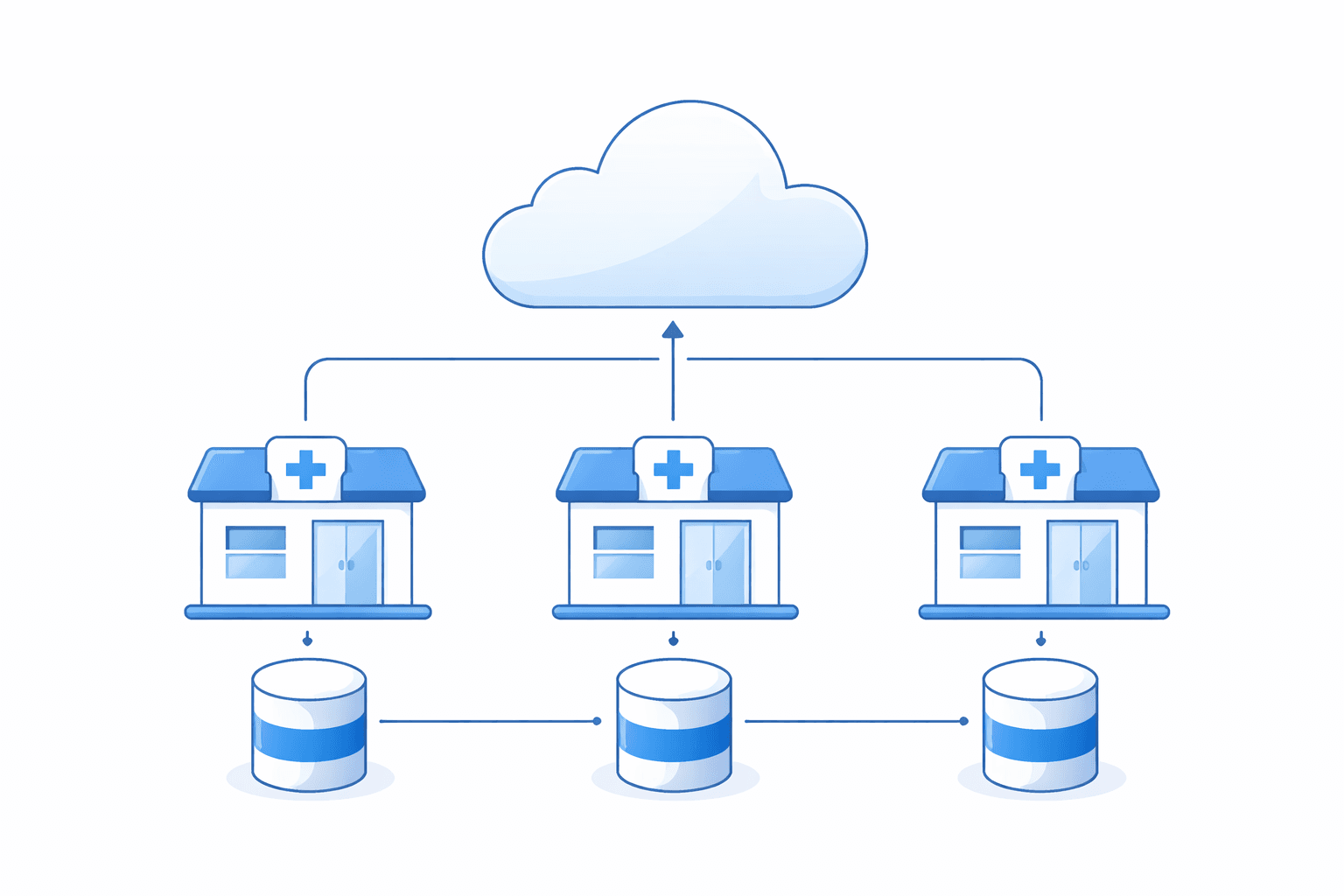
Each medical practice gets its own isolated database — deployable in any cloud region to meet local data sovereignty requirements without changing a single line of code.
Theory is one thing. Here is what it looks like in the actual architecture of doctoLys — concrete decisions made at the start of the build that made global deployment possible without ongoing country-specific engineering work.
Independent database per medical office
Rather than a shared multi-tenant database, each medical practice gets its own isolated database instance. This is the architectural foundation that solves data localization completely.
When a practice in Germany requires data residency within the EU, the database is deployed to an EU cloud region. When a practice in Saudi Arabia requires data within KSA, it deploys to a GCC region. No code change. No product adaptation. Configuration handles it.
This approach provides the maximum possible level of data isolation — particularly important in regulated healthcare environments where data sovereignty is non-negotiable.
Configurable lists for local context
Insurance plans, social security schemes, lab test catalogs, medication formularies, prescription formats, report templates — all configurable by the user, not hardcoded by the vendor.
A doctor in Morocco adds their CNSS social security scheme. A doctor in Lebanon configures their local insurance providers. A doctor anywhere builds the medication list that reflects their local formulary. The product provides the structure; the doctor fills it with their local reality.
This converts what would otherwise require 50 country-specific builds into one highly configurable product.
Workflows that mirror clinical reality, not technical architecture
The UX challenge of a universal product is significant. If the app imposes a technology-first mental model — screens organized around database tables and API schemas rather than clinical workflows — doctors will reject it regardless of technical elegance.
Every screen in doctoLys mirrors what a doctor actually does in a consultation: open a patient file, review history, record findings, write a prescription, schedule a follow-up. The sequence follows the cognitive workflow of the clinician, not the data model of the engineer. This eliminates the need for training and, with it, the need for the demo.
We examine this design philosophy in depth in an upcoming article: why mobile-first design is critical for clinical adoption.
API management for optional national integration
National integration is not part of the core product — it is an optional layer. Any practice that needs to connect to a national lab system, a patient portal, or a social security platform can do so via standard APIs.
This keeps the core product clean and universal while enabling any locally-required integration as a configuration, not a rebuild.
Generative AI as the universal language layer
Large language models are inherently multilingual. A model trained on multilingual data can transcribe a consultation in Arabic, summarize it in French, structure it according to a clinical template, and generate a prescription — without language-specific engineering.
Research on multilingual clinical AI confirms that LLMs demonstrate robust performance across languages for clinical documentation tasks — with accuracy comparable to native language models for the transcription and summarization functions that matter most in a medical office context.
In doctoLys, the AI layer handles voice transcription, consultation summarization, paper record digitization, and document structuring — across any language the doctor speaks, without configuration.
The real prerequisite: mastering both medicine and technology
The hardest part of building borderless medical software is not architectural — it is knowing what to include and what to refuse.
Every country-specific feature added is a step toward lock-in. Every hardcoded national assumption is a future barrier to a new market. Making those trade-offs consistently requires a type of expertise that is genuinely rare: someone who understands clinical workflows deeply enough to know which features are truly universal, and understands software architecture well enough to implement configurability rather than hardcoding.
Most software companies fail at this because they optimise for their largest market's feature requests without the clinical knowledge to distinguish universal needs from local administrative artifacts. A hospital billing team in Chicago asks for insurance claim processing. It gets built. It becomes a core feature. The product becomes permanently US-centric.
The insight that a solo GP in Tunisia has the same core clinical needs as a solo GP in Vietnam — and that a good product should serve both with zero country-specific code — is only available to someone who has been that doctor and also built that product.
Practical steps to evaluate if a medical product is truly borderless
If you are evaluating a medical office app for use outside its home market, here is what to look for:
- Does the product work without insurance billing, national IDs, or country-specific codes?
- Is the data storage location configurable, or fixed to the vendor's home country?
- Can you add your own medication list, insurance plans, and document templates?
- Can you self-onboard and start a consultation in under 5 minutes without speaking to anyone?
- Does the AI work in your language out of the box?
- Is there an API layer for connecting to national systems if needed?
A product that answers yes to all six was built with borderlessness as a design constraint from the beginning — not added as an afterthought.
Frequently Asked Questions
Why is most EMR software country-specific?
Most EMR platforms were built before the cloud era, when data had to live on local servers and interoperability required deep national system integration. Sales models required local representatives, and vendors optimised for their largest markets. These constraints made country-specific architecture rational at the time — but most of them no longer apply.
Is it technically possible to build medical software that works in any country?
Yes. Database-per-tenant deployment solves data localization. FHIR provides a global interoperability standard. LLMs handle multilingual transcription and documentation. The technical barriers have largely disappeared — what remains is a product philosophy challenge.
What is FHIR and why does it matter for global medical software?
FHIR (Fast Healthcare Interoperability Resources) is the global standard for healthcare data exchange — a RESTful API that allows any healthcare system to communicate with any other, regardless of country. A product built on FHIR can integrate with any national platform as a configuration rather than a rebuild.
How does data localization work in a borderless medical app?
A database-per-tenant architecture gives each practice its own isolated database instance, deployable in any cloud region — EU, GCC, Asia-Pacific — to comply with national data sovereignty laws without changing the application code. The product is the same everywhere; the data location is configurable.
Why does targeting a global market produce better pricing for doctors?
A software company targeting only the US or European market voluntarily ignores hundreds of millions of physicians worldwide. A larger total addressable market allows the developer to invest more in the product and offer lower pricing — $19/month becomes viable when the addressable user base is global, not regional.
A medical office app built for the world
doctoLys was designed from day one with zero country dependencies.
Written by Dr. Sadok Derouich, a practicing gynecologist since 2012, digital health entrepreneur, and CEO of doctoLys — the AI medical office app built for doctors worldwide.
Further Reading
March 13, 2026
Why most EMR software fails outside the US and Europe
The market was built for Western doctors. Here is why that excludes most of the world — and what the data shows about adoption failure rates.

March 15, 2026
Can a mobile-first app solve the EMR adoption crisis in developing countries?
Why the smartphone is the bridge that PC-based EMRs never built — and what a truly mobile-first medical office app looks like.

About the Author
Dr. Sadok DerouichDr. Sadok Derouich is a practicing gynecologist since 2012, digital health entrepreneur, and CEO of Doctolys — the AI medical office app built for doctors worldwide.
View Derouich's profile →Stay Updated
Get the latest insights on AI in medicine delivered to your inbox.